مجلات علمية





The branches of coronary arteries anatomy
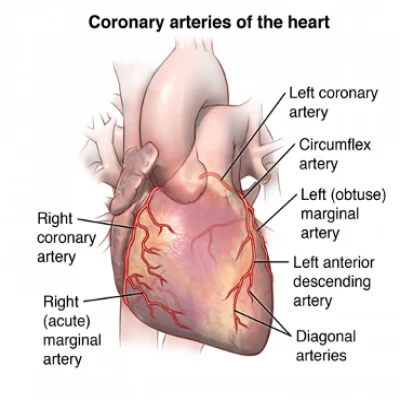
Coronary arteries are supplied with blood via coronary arteries. The heart muscle, like all other body tissues, demands oxygen-rich blood to operate. Additionally, oxygen-depleted blood must always be transported. The coronary arteries surround the heart on all sides. To supply blood to the heart muscle, little branches dive into it1.
Coronary arteries anatomy1
What do the various coronary arteries look like?
The left main and right main coronary arteries are the two primary coronary arteries.
The coronary artery on the left side is called the left major coronary artery (LMCA). Blood is supplied to the left side of the heart muscle by the left major coronary artery (the left ventricle and left atrium). The coronary artery in the left main separates into different sides1:
· The left anterior descending artery is a branch of the left coronary artery that provides blood to the heart's front side.
· The circumflex artery is a branch of the left coronary artery that runs around the heart muscle. This artery sends blood to the heart's exterior and back sides.
Coronary artery to the right (RCA). The right coronary artery feeds the right ventricle, right atrium, and the SA (sinoatrial) and AV (atrioventricular) nodes, which control heart beat. The right posterior descending artery and the severe margin artery are two minor branches of the right coronary artery. The right coronary artery, along with the left anterior descending artery, assists to provide blood to the heart's centre or septum.
The obtuse marginal (OM), septal perforator (SP), and diagonals are smaller segments of the coronary arteries.
Branches
The designated parts of the coronary circulation in a right-dominant heart are as follows2:
· Left coronary artery (LCA) / Left major coronary artery (LMCA) Aorta Left circumflex artery (LCX)
· Marginal artery #1 is obtuse (OM1)
· Second obtuse marginal artery (OM2)
· The artery that runs down the left side of the body is called the left anterior descending (LAD)
· #1 Diagonal Artery
· #2 Diagonal Artery
· Coronary artery to the right (RCA)
· Nodal branch of the atrioventricular node
· artery of the right marginal
· The artery that runs down the back of your neck is called the posterior descending artery (PDA)
· PL#1 (posteriolateral artery #1)
· PL#2 (posteriolateral artery #2)
Anatomy of the Coronary
Veins of the heart
Cardiac veins are the channels that evacuate deoxygenated blood from the heart tissue. The great heart vein, middle heart vein, small heart vein, tiniest cardiac veins, and anterior heart veins are among them. Heart veins transport oxygen-depleted blood from the heart to the right atrium. The coronary sinus is where the majority of the blood from the coronary veins circulates. The great heart vein, the middle cardiac vein, the small cardiac vein, the posterior vein of the left ventricle, and the vein of Marshall are heart veins that go into the coronary sinus. The anterior ventricular veins, the tiniest heart veins, flow straight to the right atrium (Thebesian veins).3
What is collateral rotation, and how does it work?
Collateral circulation is a network of small blood arteries that are normally closed. Collateral veins may grow by becoming active when coronary arteries narrow to the point that blood supply to the heart muscle is restricted (coronary artery disease). This pumps the blood around the blocked artery and into another neighbouring artery or the same artery past the obstruction, sparing the heart tissue4.
Collateral vessels surround blocked blood vessel4
What is the significance of coronary arteries1?
Because coronary arteries supply blood to the heart muscle, any coronary artery condition or disease that reduces the delivery of oxygen and nutrients to the heart muscle might have catastrophic consequences. This can result in a cardiac arrest and death. The most prevalent cause of heart disease was atherosclerosis (plaque buildup in the inner lining of an artery that causes it to narrow or get clogged).
The most prevalent cause of artery narrowing is atherosclerosis, also known as arteriosclerosis or arteriolosclerosis. Plaques (deposits of cholesterol and other chemicals) build up in the walls of the blood vessels throughout time, causing blockages. The shrinking of the coronary arteries is referred to as coronary artery disease (CAD) or ischemic heart disease (IHD).5
Plaque development can partly obstruct blood supply to the heart muscle as the condition advances. The heart can't perform correctly if it doesn't get enough blood (ischemia), especially when it's under a lot of pressure. Fixed angina is chest pain that gets better with relaxation. Unstable angina is chest discomfort that occurs at relaxation, is more severe than stable angina, and lasts longer. It's caused by a worsening of artery narrowing.6
A heart attack happens when a plaque fractures and a thrombus (blood clot) forms, obstructing flow of blood to a part of the heart and causing tissue death (infarct).
Cardiac arrest or arrhythmias can also be caused by CAD. Chronic oxygen deprivation owing to diminished blood flow causes heart disease, which weakens the heart over time. Arrhythmias are caused by a lack of blood supply to the heart, which interferes with the electric impulse of the heart.
The coronary arteries can contract in reaction to a variety of stimuli, the majority of which are chemical. A coronary reflex is what this is called.
Spontaneous coronary artery anatomy is a rare disorder in which the wall of one of the blood vessels breaks, causing intense pain.
With the exception of CAD, spontaneous coronary artery anatomy is caused by a buildup of plaque in the arteries and is more common in younger people, such as females who have recently had a baby or males who engage in intensive activity.7
Atherosclerosis8
Coronary Anomalies9
Coronary abnormalities are rare, with just 1% of people suffering from them.
Due to their possible link to myocardial ischemia and unexpected mortality, early diagnosis and assessment of coronary artery abnormalities is critical10.
We will have more of these abnormalities as the usage of cardiac-CT increases.
Abnormalities of the origin, course, and termination are the three types of coronary anomalies.
The most prevalent and clinically significant abnormality is depicted in the left top corner.
The LCA has an unusual origin from the right sinus of Valsalva, and it runs between the aorta and the pulmonary veins.
The LCA (yellow arrows) may be compressed as a result of this interarterial route, leading in myocardial ischemia.
The left-hand anomalies aren't hemodynamically significant.
Coronary Anomalies9
The coronary arteries run along the coronary sulcus of the myocardium of the heart. Their main function is to supply blood to the heart. This is a crucial function for myocardial function and subsequently homeostasis of the body. The arrangement of coronary arteries varies among people significantly11.
1. https://en.wikipedia.org/wiki/Coronary_circulation
4. https://my.clevelandclinic.org/health/articles/17063-coronary-arteries
5. "Coronary Artery Disease: Causes, Diagonosis & Prevention| cdc.gov". www.cdc.gov. 2018-10-09. Retrieved 2019-09-01.
6. ^ "Coronary Artery Disease". Cleveland Clinic. Retrieved 2019-09-01.
7. ^ "Coronary Artery Dissection: Not Just a Heart Attack". www.heart.org. Retrieved 2019-09-02.
8. https://en.wikipedia.org/wiki/Coronary_arteries
9. https://radiologyassistant.nl/cardiovascular/anatomy/coronary-anatomy-and-anomalies
10.Visualization of Anomalous Coronary Arteries on Dual Source Computed Tomography by G.J. de Jonge et al European Radiology, Volume 18, Number 11 / November, 2008, 2425-2432