مجلات علمية





What is Pathology?
Pathology is the investigation of the circumstances and end results of illness or injury. The word pathology additionally alludes to the investigation of infection by and large, joining a wide scope of science research fields and clinical practices. In any case, when utilized with regards to current clinical therapy, the term is regularly utilized in a tighter manner to allude to cycles and tests which fall inside the contemporary clinical field of "general pathology", a region which incorporates various unmistakable however between related clinical claims to fame that analyze illness, for the most part through investigation of tissue, cell, and body liquid examples. Informally, "a pathology" may likewise allude to the anticipated or real movement of specific sicknesses (as in the assertion "the a wide range of types of malignant growth have assorted pathologies", in which case a more appropriate decision of word would be "pathophysiologies"), and the join pathy is in some cases used to show a condition of illness in instances of both actual affliction (as in cardiomyopathy) and mental conditions, (for example, psychopathy). A doctor rehearsing pathology is known as a pathologist1.
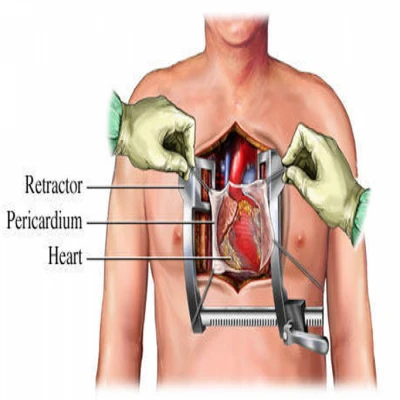
A pathologist looks at a tissue area for proof of destructive cells while a specialist notices2.
Heart Pathology
'Obsessive' cardiovascular hypertrophy is a condition that is portrayed by the thickening of the heart muscle, a lessening in the size of the loads of the heart, and a decreased limit of the heart to siphon blood to the tissues and organs around the body. Two normal reasons for obsessive cardiovascular hypertrophy are (hypertension) and heart valve stenosis, and this sort of hypertrophy is viewed as a significant autonomous danger factor for horribleness and mortality. Then again, 'physiological' heart hypertrophy can be incited by practice preparing and can prompt increment cardiovascular size that is portrayed by ordinary cardiovascular morphology with a typical and additionally improved cardiovascular capacity3. Furthermore, practice preparing has been demonstrated to be the main commonsense and supportable countermeasure equipped for giving cardioprotection by working on myocardial resilience to ischaemia–reperfusion injury (for example coronary failure)4.
Albeit the two kinds of cardiovascular hypertrophy are started by an over-burden to the heart, the particular contrasts between the two can be ascribed to the sort of over-burdening upgrades. Nonetheless, information likewise involve term and force of the heart over-burden in deciding if the cardiovascular hypertrophy that creates is 'obsessive' or 'physiological'. Without a doubt, even the advantages of activity can be portion subordinate. For instance, extremely focused energy/span exercise can result in negative cardiovascular primary and electrical heart renovating.
Patent Ductus Arteriosus
Cardiovascular pathologies are a significant reason for bleakness and mortality. Treatment choices have grown essentially lately. Albeit the standards of cardiovascular medical procedure and interventional cardiology, for example, entering heart injury list (PTCI), coronary vein sidestep joining, valve and vascular medical procedure, have stayed unaltered for quite a long time, significant specialized improvements have showed up. Mechanical technology and negligibly intrusive strategies limit or take out the time spent on cardiopulmonary detour (CPB). Half breed cardiovascular medical procedure could offer and join methodology, like PTCI and off-siphon coronary conduit sidestep (OPCAB), percutaneous valve substitution valve and negligibly intrusive direct coronary corridor sidestep (MIDCAB), or insignificantly obtrusive valve fix. Such methods offer various methodologies to achieve interventional cardiovascular consideration while remaining insignificantly intrusive5.
Various cardiovascular pathologies can make the heart go through delayed scenes of raised responsibility, which if inordinate can prompt a hypertrophic reaction, causing growth of the heart. While cardiovascular hypertrophy can be a typical physiological reaction to practice in solid grown-ups and isn't harming to the heart, neurotic hypertrophy (whenever supported over the long run) is harming and will ultimately prompt a decrease in LV capacity and to HF6. Two sorts of hypertrophy have been portrayed. Concentric hypertrophy is because of constant tension over-burden, where there is an expansion in divider thickness because of expansion of equal sarcomeres causing an increment in cardiomyocyte width. This permits the cardiomyocytes at first to produce more power and lessen tension on the myocardium. Be that as it may, with sickness movement cardiomyocyte demise happens and heart fibrosis expands, prompting myocardial firmness and cardiovascular brokenness. Flighty hypertrophy is brought about by volume over-burden and prompts divider diminishing and dilatation of the heart. The cardiomyocytes again go through an adjustment of shape, this time becoming stretched through the expansion of sarcomeres in series. As infection advances cardiomyocytes are lost through apoptosis, prompting divider diminishing, heart dilatation and loss of cardiovascular contractility. These progressions fit as a fiddle are directed by the idea of the over-burden measure. It ought to likewise be noticed that these cycles are not totally unrelated and obsessive cardiovascular hypertrophy frequently advances to expanded cardiomyopathy7.
A heart attack in progress. Animation screenshot from Physiology & Pathology8.
Basic Cardiac Pathology
The prohibition of heart pathology as a contributing variable in SUDEP is trying because of the presence of, for instance, unpretentious anomalies that main a nitty gritty minuscule assessment of cardiovascular tissue can clarify, like directing framework fibrosis or cardiomyopathy,79 tissue deterioration blocking the obtaining of reasonable material for assessment, absence of a fitting benchmark group for correlation, and the chance of a utilitarian instead of an underlying problem, for example, particle channelopathies or preexcitation conditions, with ordinary plainly visible and tiny assessments being implicated.43 Furthermore, irregularities in the approach and announcing of cardiovascular irregularities in SUDEP after death reports forestall significant examination of results9.
Adiponectin in heart Disease as an Antiinflammatory Protein
In the advancement of intense cardiovascular pathology like myocardial localized necrosis and congestive cardiovascular breakdown, adiponectin is an intense stage reactant. A convergence of HMW adiponectin is seen in harmed myocardial tissue and expanded adiponectin was estimated in blood during intense cardiovascular breakdown. After the intense stage, HMW/all out adiponectin proportion diminished. Truth be told, constant cardiovascular pathology, for example, remunerated cardiovascular breakdown is contrarily connected with HMW and absolute adiponectin fixation, with a more grounded negative affiliation creating as seriousness of CVD advances10.
The improvement of atherosclerosis and resulting myocardial ischemia is portrayed by reformist aggravation and endothelial brokenness. HMW and absolute adiponectin have different antioxidative and calming impacts in this cycle.
In the intense cardiovascular setting, there is close association among adiponectin and the inborn safe framework. Adiponectin is primarily like C1q and is equipped for enacting the old style supplement pathway by restricting to C1q through the globular space of the C1q A-chain. C1q-adiponectin edifices circle in blood and have been emphatically connected with atherosclerosis and intense coronary disorder. Moreover, in the last mentioned, C1q-adiponectin edifices were found in perivascular spaces of fat tissue and in the intimal-media layer of the supply route11.
Suggested mechanism of adiponectin (AdN) regulation in cardiovascular disease (CVD). In healthy/early CVD adipose tissue (left ventricular ejection fraction [LVEF] >50%), adiponecting (AdN) release is suppressed by low-grade inflammation and low AdN levels predict for CVD onset. In advanced CVD (LVEF <35%) adipose, the balance is shifted toward brain natriuretic peptide (BNP)-mediated increased AdN release and high AdN levels can predict poor prognosis in these patients12.
Coronary illness, any issue of the heart. Models incorporate coronary illness, inborn coronary illness, and pneumonic coronary illness, just as rheumatic coronary illness (rheumatic fever), hypertension, irritation of the heart muscle (myocarditis) or of its internal or external layer (endocarditis, pericarditis), and heart valve sickness. Irregularities of the heart's regular pacemaker or of the nerves that direct its driving forces cause arrhythmias. Some connective tissue sicknesses (strikingly foundational lupus erythematosus, rheumatoid joint pain, and scleroderma) can influence the heart. Cardiovascular breakdown might result from a significant number of these problems13.
Important to understand how cardiovascular physiology is entwined with other organ frameworks and how pathophysiology relates back to straightforward gross physiology. Heart physiology is one of the main bits of clinical information in medical care. The cardiovascular framework is continually adjusting to keep up with homeostasis in the body, explicitly to keep up with oxygen perfusion of tissues. The heart will adjust by means of numerous factors, for example, pulse, stroke volume, preload, afterload, diastole, and systole. This article characterizes these terms and extrapolates them into a functioning model of heart physiology14.
References
1. "-pathy, comb. form: Oxford English Dictionary". OED Online (3rd ed.). Oxford University Press. 2005. Retrieved 23 March 2020.
2. https://en.wikipedia.org/wiki/Pathology
3. Ooi JY, Bernardo BC. McMullen JR. The therapeutic potential of miRNAs regulated in settings of physiological cardiac hypertrophy. Future Med Chem. 2014; 6:205–222.
4. Powers SK, Smuder AJ, Kavazis AN. Quindry JC. Mechanisms of exercise-induced cardioprotection. Physiology (Bethesda) 2014; 29:27–38.
5. Modine, T. (2012). Minimized Cardiopulmonary Bypass Techniques and Technologies || Minimally invasive cardiac surgery, port-access and robotic surgery., (), 229–244. doi:10.1533/9780857096029.3.229
6. Wakatsuki , T. , Schlessinger , J. and Elson , E.L. 2004 . The biochemical response of the heart to hypertension and exercise. Trends Biochem Sci 29: 609 – 17.
7. Lorell , B.H. , and Carabello , B.A. 2000 . Left ventricular hypertrophy: pathogenesis, detection, and prognosis. Circulation 102 : 470 – 9 .
8. https://www.visiblebody.com/blog/physiology-pathology-four-common-cardiovascular-conditions
9. https://www.sciencedirect.com/science/article/abs/pii/B9781416061717000157
10. K.W. Liang, W.J. Lee, W.L. Lee, C.T. Ting, W.H. Sheu, decreased ratio of high-molecular-weight to total adiponectin is associated with angiographic coronary atherosclerosis severity but not restenosis, Clin. Chim. Acta 405 (1–2) (2009) 114–118.
11. E.S. Hong, C. Lim, H.Y. Choi, E.J. Ku, K.M. Kim, J.H. Moon, S. Lim, K.S. Park, H.C. Jang, S.H. Choi, The amount of C1q-adiponectin complex is higher in the serum and the complex localizes to perivascular areas of fat tissues and the intimal-medial layer of blood vessels of coronary artery disease patients, Cardiovasc. Diabetol. 14 (2015) 50.
12. https://www.ahajournals.org/doi/full/10.1161/atvbaha.114.304380
13. https://www.britannica.com/science/heart-disease
14. Oberman R, Bhardwaj A. Physiology, Cardiac. [Updated 2021 Jul 21]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK526089/